
The G-spot is not a hidden button waiting to be found — it’s a region of overlapping anatomy that responds to the right kind of pressure, not a precise address.
The real source of internal pleasure isn’t a single spot; it’s a network — and understanding that changes everything about how g-spot stimulation actually works.
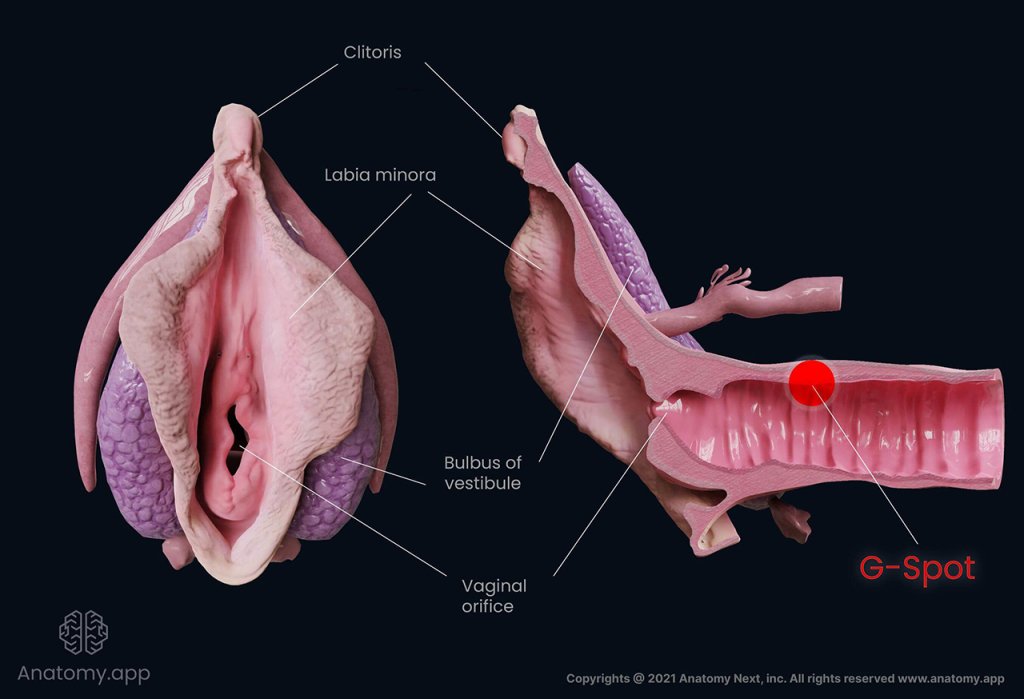
The G-spot as a region: According to The Journal of Sexual Medicine, the G-spot is not a distinct anatomical structure but an extension of the clitoral network located on the anterior vaginal wall — roughly one to three inches inside, toward the belly button. What researchers have consistently found is that this area is dense with nerve endings, erectile tissue, and vascular structures that respond collectively to stimulation. There is no single anatomical “spot” that lights up independently.
The clitoral network connection. The internal roots of the clitoris — a much larger organ than the external nub most people recognize — extend deep into the pelvic region and run adjacent to the anterior vaginal wall. When pressure is applied to that front wall, it indirectly engages those internal clitoral roots. This is why some positions and angles produce dramatically more sensation than others: they’re reaching the clitoral network from the inside.
Pressure over precision. Because the responsive tissue spans a region rather than a pinpoint, the common frustration of “not being able to find it” often comes from applying too little pressure or using the wrong angle rather than missing a specific location. Firm, consistent, curved pressure against the anterior wall is what activates this tissue — which is exactly why the anatomy of the G-spot matters before discussing technique. That tissue also has a close relationship with the Skene’s glands, which plays a significant role in what happens when stimulation intensifies.
Skene’s Glands and the Science of Female Ejaculation
Understanding what actually happens inside the body during G-spot stimulation transforms the experience from mystery into measurable physiology — and Skene’s gland anatomy is the key to that understanding.
The Skene’s glands, often called the “female prostate,” are a pair of small glandular structures located on the anterior wall of the vagina, flanking the urethral opening. Their tissue composition closely mirrors that of the male prostate, producing similar proteins and responding to the same kind of sustained pressure. This isn’t coincidence. Research increasingly supports the idea that the Skene’s glands are the primary anatomical driver behind both deep G-spot sensation and female ejaculation.
When firm, rhythmic pressure is applied to the anterior vaginal wall — exactly the region Dr. Jess O’Reilly describes as “an area of highly sensitive tissue that, when stimulated, can lead to powerful, full-body orgasms” — the Skene’s glands begin to engorge with fluid. This engorgement is what creates the characteristic “fullness” many people report during G-spot stimulation. As arousal intensifies and pressure continues, that fluid can be released through the urethral opening. This is female ejaculation: a documented, physiologically normal response, not an anomaly or an accident.
The sensation tied to Skene’s gland activation tends to be qualitatively different from clitoral stimulation. Rather than a localized surface response, it often radiates through the pelvic floor and lower abdomen — what researchers and clinicians describe as a diffuse, full-body experience. Some individuals also report a brief urge to urinate just before climax, which is a normal result of pressure on urethral-adjacent tissue, not a signal to stop. Knowing this removes a common source of hesitation and allows the body to respond without interruption.
Female ejaculation remains underresearched relative to male sexual response, but the existing scientific literature consistently frames it as a natural physiological process. Normalizing it matters — because hesitation and self-consciousness are among the most common barriers to the kind of sustained, consistent stimulation the Skene’s glands actually require to fully activate. And that consistency, it turns out, is very much a question of mechanics.
Why the ‘Come Hither’ Motion Requires Ergonomic Engineering
Manual G-spot stimulation demands a very specific physical action — and the human hand, despite its dexterity, is fundamentally ill-equipped to sustain it.
The classic technique involves inserting one or two fingers, palm-facing-up, and curling them toward the belly button in a slow, firm, rhythmic motion. This “come hither” gesture directs pressure precisely at the anterior vaginal wall, where the erectile tissue surrounding the G-spot responds to sustained compression rather than fleeting touch. The motion sounds straightforward, but executing it effectively is challenging.
The wrist joint wasn’t designed for this work. Maintaining upward-angled pressure at 2–3 inches inside the vaginal canal requires awkward wrist flexion sustained over several minutes — and as fatigue sets in, pressure becomes inconsistent. Muscle tremors reduce precision. The angle drifts. What began as targeted stimulation gradually loses the mechanical reliability that pelvic floor sensitivity actually requires. According to Lioness, many people simply can’t apply enough consistent pressure manually to produce a reliable response.
Ergonomic toy design addresses these limitations directly. Three mechanical advantages define purpose-built G-spot tools:
- Curved or hooked profile — A pronounced C-shaped curve positions the stimulating head at the anatomically correct angle without requiring wrist contortion, keeping pressure fixed on the anterior wall throughout use.
- Rigid or semi-rigid body — Unlike flexible straight insertables, firmer construction transmits force efficiently rather than absorbing it, ensuring that each motion actually reaches deep tissue.
- Consistent applied pressure — Mechanical delivery eliminates the fatigue variable, maintaining the steady rhythmic contact that unlocks cumulative arousal responses more reliably than manual effort can.
For those exploring depth-based stimulation beyond the G-spot — the A-spot sits even further along the anterior wall — ergonomic reach becomes even more critical. But the core principle holds at every level: the body responds to consistency, and consistency demands the right tool. That insight naturally raises a question about what kind of mechanical action works best — and whether vibration alone is truly the most effective delivery method.
The Evolution of Pleasure: Automated Tapping vs. Standard Vibration
Standard vibration technology — the foundation of most conventional devices — often works against the very biology it’s designed to stimulate. When high-frequency buzz is applied continuously to sensitive tissue, mechanoreceptors in the area become habituated, a process sometimes called vibratory desensitization. Prolonged surface vibration doesn’t build toward climax; it can actively dull the deep nerve pathways that G-spot stimulation depends on. The anterior vaginal wall requires rhythmic, targeted pressure to engage the urethral sponge and the internal clitoral complex, rather than constant surface-level hum.
This is where tapping technology represents a genuine mechanical leap. Rather than emitting a steady buzz, tapping mechanisms deliver rapid, percussive pulses that replicate the rhythmic pressure of deliberate manual stimulation — the very motion that the “come hither” technique mimics. This is significant because the Skene’s glands and surrounding erectile tissue respond more effectively to intermittent compression than to sustained vibration, which connects directly to the female ejaculation science explored earlier in this article. Research consistently shows that the G-spot region involves complex neurovascular tissue that benefits from varied, pressure-based input rather than monotonous frequency.
Multi-functional devices take this engineering a step further. A well-designed 3-in-1 stimulator can deliver internal tapping, external clitoral suction, and targeted vibration simultaneously — addressing the full anatomical picture rather than isolating a single sensation. As noted by Healthline, curved C-shaped or hooked devices are anatomically superior for G-spot work because their geometry naturally maintains contact with the anterior wall during use. Kissself has built on this principle, engineering devices that combine precision curvature with automated tapping rhythms — a mechanical innovation that moves sexual wellness technology closer to what human touch actually does. Understanding how the body receives this stimulation is only half the equation, though — how you prepare internally before and after use plays an equally important role, which brings us to the pelvic floor.
Pelvic Floor Sensitivity: Preparing the Body for Internal Pleasure
The pelvic floor is the often-overlooked gatekeeper of G-spot sensation — its state of tension or relaxation directly determines how much pleasure is accessible during internal stimulation.
Tension and relaxation aren’t opposites here; they’re partners that need to be properly sequenced.
Relaxation First
Before any form of G-spot work begins, the pelvic floor must be in a receptive state. A common pattern is that people attempt internal stimulation while still physically guarded — muscles braced, arousal incomplete. This creates a counterproductive cycle. When the pelvic floor is hypertonic (chronically tight), the anterior vaginal wall becomes less accessible and more resistant to pressure. According to research on orgasm and stimulation, approximately 18% of women report reaching orgasm through vaginal penetration alone, while the majority require combined or indirect clitoral stimulation — a figure that becomes even more relevant when pelvic floor tension is reducing internal sensitivity. Arousal, slow breathing, and adequate foreplay aren’t optional steps; they’re physiological prerequisites.
Working With Tension
On the other hand, a pelvic floor that has been brought to a moderate level of voluntary engagement — not bracing, but active — can actually amplify G-spot sensations. This is where automated devices with rhythmic, repeating motions offer a genuine advantage. A curved g-spot wand with a consistent tapping or pulsing action can serve as a kind of internal myofascial release tool, helping hypertonic muscles soften through gentle mechanical repetition. In practice, this gradual desensitization of tight tissue can make the anterior wall progressively more responsive over a session. Pairing device use with paced exhales — keeping exhales slightly longer than inhales — supports this process, as outlined in breath-pacing guidance for pelvic floor sensitivity.
Integration and Climax
Pelvic floor health directly shapes the ceiling of orgasmic intensity. A well-conditioned, responsive pelvic floor generates stronger involuntary contractions during climax — the physical mechanism behind what many describe as a “deeper” or more full-body orgasm. Building this foundation through consistent awareness of relaxation and engagement patterns doesn’t just improve any single session; it compounds over time. Once the body learns to move fluidly between release and activation, the conditions for sustained, intense G-spot stimulation become far more reliable — setting the stage for how physical positioning can further refine that experience.
Optimizing Your Experience: Positions for Targeted Stimulation
Body positioning is one of the most underrated variables in G-spot access — a small angle adjustment can mean the difference between near-miss stimulation and direct, consistent contact.
As established earlier, the G-spot sits on the anterior wall of the vagina, typically 2–3 inches inside. Because that location is fixed, you control the equation by changing the geometry around it. Here’s how positioning translates into practice:
Coital Alignment Technique (CAT) for partner play. CAT shifts the partner’s body slightly upward so the base of the penis or toy maintains friction against the anterior vaginal wall throughout each movement. Unlike standard missionary, it keeps consistent anterior pressure while simultaneously engaging the clitoral network — a key reason it’s associated with higher rates of blended orgasm during partnered sex.
Legs elevated for solo exploration. Lying on your back and drawing the knees toward the chest — or resting legs against a wall — tilts the pelvis and shortens the effective depth of the vaginal canal. This naturally angles the anterior wall downward and makes it significantly easier to apply upward, “come hither” pressure with fingers or a curved device. Many people find this the most intuitive starting position.
Seated or reclined use of a curved wand. In a seated position with hips slightly forward, gravity assists anterior wall contact without requiring you to hold an awkward angle. Reclining at roughly 45 degrees achieves a similar effect. For both positions, guiding the curve toward the navel — not straight in — is the critical cue. If you’re exploring rear-entry angles with a partner, the same navel-direction principle applies.
For visual learners, the tutorial below walks through these positions with clear anatomical context:
[YOUTUBE VIDEO EMBED PLACEHOLDER]
Small positional shifts are where science meets sensation — and they set the stage for understanding why the research community’s ongoing debate about G-spot anatomy matters far less than your personal experience of that pleasure zone.
A Systematic Review: Fact vs. Fiction in Medical Literature
The scientific debate over the G-spot isn’t about whether pleasure exists there — it’s about what to call the anatomy producing it. A 2021 systematic review published in PMC examined decades of anatomical and clinical research and reached a nuanced conclusion: no discrete, universally identifiable organ called the “G-spot” could be isolated in cadaveric or imaging studies. However, the anterior vaginal wall consistently emerged as a high-sensitivity region capable of producing intense pleasure responses — a distinction that matters far more in practice than in terminology.
The real finding isn’t absence of sensation — it’s absence of consensus on naming it. The review highlights a genuine split between researchers who argue for a distinct erogenous structure and those who classify the response as an extension of internal clitoral tissue. What both camps agree on, however, is that stimulation of this anterior zone produces documented physiological responses in many people, including increased arousal, vaginal engorgement, and in some cases, ejaculatory fluid release from the Skene’s glands. Whether that makes it a “spot” or a “zone” is a question of anatomy textbooks, not lived experience. Interestingly, similar debates around lesser-known internal erogenous regions — explored in detail here — show that nomenclature consistently lags behind what bodies are already doing.
The practical takeaway from the scientific literature is straightforward: personal experience outweighs clinical nomenclature every time. If stimulation of a specific internal region produces pleasure, that response is real and valid — regardless of whether a future anatomy atlas gives it a formal name. The ongoing academic debate is actually a healthy sign that researchers are taking this region seriously after decades of dismissal. For anyone navigating their own body, the consensus that matters most is the one formed through attentive, informed self-exploration — which is precisely what the right tools and techniques make possible.
The Bottom Line: Master Your Internal Pleasure
Understanding G-spot stimulation becomes straightforward once you stop searching for a hidden button and start treating it as a region of interconnected anatomy that responds to the right tools, angles, and awareness.
The G-spot is not a standalone structure — it’s a functional zone of the clitoral network, including internal clitoral tissue, the urethral sponge, and Skene’s glands working in concert. As sex educator Dr. Jess O’Reilly has noted, the “fiction” of the G-spot often stems from people looking for a tiny, specific point rather than engaging a broader responsive area. That framing shift alone changes everything about how you approach exploration.
Curved wands are non-negotiable for accessing the anterior vaginal wall consistently. A straight toy simply cannot apply upward pressure against that ridged tissue with the same precision. This is why purpose-designed geometry matters more than raw power or size. And when it comes to the rhythm of stimulation, mechanical tapping — the kind delivered by automated pleasure technology — creates a repeatable, consistent pressure pattern that manual fingers struggle to sustain over time. Fatigue, angle drift, and inconsistent speed all interrupt the buildup that G-spot response requires.
Equally important is what happens before stimulation begins. A relaxed pelvic floor allows the tissue to soften and become more accessible. Arousal increases blood flow to the area, making the urethral sponge more prominent and easier to locate. Many people find that post-orgasm sensitivity following G-spot stimulation feels distinctly different from clitoral orgasm — a fuller, deeper sensation tied to that internal network.
Female ejaculation, if it occurs, is a normal physiological response to Skene’s gland stimulation — not an accident, not a problem. The systematic review published in PMC supports this as a well-documented phenomenon, distinct from urinary incontinence and worthy of destigmatization.
With this foundation in place, the questions that remain tend to be practical ones — and those are exactly what the next section addresses directly.
Frequently Asked Questions About G-Spot Exploration
Precision G-spot stimulation is one of the most searched and least clearly answered topics in sexual wellness — so these five questions cut straight to what matters most.
Where is the G-spot located exactly?
The G-spot sits on the anterior (front) wall of the vagina, roughly 2–3 inches inside. According to research reviewed on Apple Podcasts’ Science Vs, it’s best understood as a region of erectile tissue connected to the internal clitoris, rather than a single fixed point. Using a “come hither” finger curve toward the belly button is the most reliable way to locate it.
Can everyone have a G-spot orgasm?
Not everyone reaches G-spot orgasm in the same way or at all, and that’s completely normal. As Cosmopolitan notes, this area of highly sensitive tissue can produce powerful, full-body orgasms when stimulated — but anatomy, arousal level, and comfort all influence the outcome. Consistent exploration without pressure tends to deliver the best results over time.
Is female ejaculation the same as peeing?
No — though it can feel similar due to shared anatomical pathways. Female ejaculation originates from the Skene’s glands, not the bladder, and its fluid composition differs from urine. If you’re curious about indirect stimulation routes that can also engage this region, those are worth exploring too.
What is the best toy for G-spot stimulation?
A curved vibrator with a firm, angled head designed to maintain contact with the anterior vaginal wall outperforms flat or straight designs. The upward curve replicates the manual “come hither” motion, providing consistent pressure and reach.
How long does it usually take to find it?
There’s no universal timeline. Some people locate it within minutes; others need several exploratory sessions as arousal increases blood flow and tissue engorgement. It’s also worth knowing that heightened sensitivity post-orgasm is normal and doesn’t mean stimulation went wrong — it means it went right.