If you’re wondering how to have multiple orgasms as a man, the most realistic, science‑backed path is to train arousal regulation and ejaculation control while keeping safety front and center.
Key takeaways for how to have multiple orgasms
- Multiple orgasms for AMAB people are possible for some, but not guaranteed. Aim to separate orgasm sensations from ejaculation and extend arousal rather than chase a fixed outcome.
- Master the basics first: understand orgasm versus ejaculation, the refractory period, and why timing and breath matter.
- Use behavior methods like start–stop and pause–squeeze to learn when to ease off, then return to a pleasurable plateau.
- Train pelvic‑floor control and full relaxation, not just hard contractions; overtraining can backfire.
- Consider gentle, optional prostate stimulation with strict hygiene and barrier practices if you explore that path.
- Track sessions, progress slowly over 4–8 weeks, and seek clinical advice if you experience pain, bleeding, or persistent dysfunction.
The physiology that makes or breaks multiple orgasms
Orgasm and ejaculation are linked but separable events. Patient education resources explain that orgasm can occur without semen release in conditions such as anejaculation, which is distinct from not orgasming at all. They also describe retrograde ejaculation, where semen flows into the bladder while orgasmic sensation remains. See the Cleveland Clinic overviews of anejaculation and retrograde ejaculation as definitional context.
- According to the Cleveland Clinic’s plain‑language explainer on the sexual response cycle, the post‑orgasm refractory period varies widely by person, age, and health, which is why back‑to‑back orgasms can be difficult for many. Read the section on the refractory period in the Cleveland Clinic’s Sexual Response Cycle guide: Cleveland Clinic sexual response cycle overview.
- For definitions that distinguish orgasm sensation from semen release, see the Cleveland Clinic’s patient pages on anejaculation and orgasm without semen expulsion and retrograde ejaculation and dry orgasm.
- Mechanism myths persist. Animal research published in 2021 suggests prolactin may not be the on‑off switch for the refractory period; human data remain limited. See the peer‑reviewed discussion in Valente et al., 2021: Prolactin and the post‑ejaculatory refractory period.
Bottom line: learning how to have multiple orgasms is really about reading your own arousal, pausing before the “point of no return,” and sometimes exploring non‑ejaculatory peaks. Your refractory period still matters, so plan training sessions with rest.
Training plan for how to have multiple orgasms
The timeline below emphasizes skill building rather than guaranteed outcomes. Use lube, privacy, and a relaxed setting. If you feel pain or distress, stop.
Weeks 1 to 2 foundation
Objective: Map arousal levels and practice coming down from high arousal without ejaculating.
- Arousal mapping: During solo play, rate your arousal from 1 to 10. Each time you reach 7 to 8, stop stimulation, unclench your jaw, drop your shoulders, and breathe out slowly for 30 to 60 seconds. Resume at a gentler pace once the edge passes.
- Start–stop familiarization: Do 2 to 3 cycles per session, 2 to 3 sessions a week. Keep the focus on sensing the “point of no return,” not on delaying at any cost.
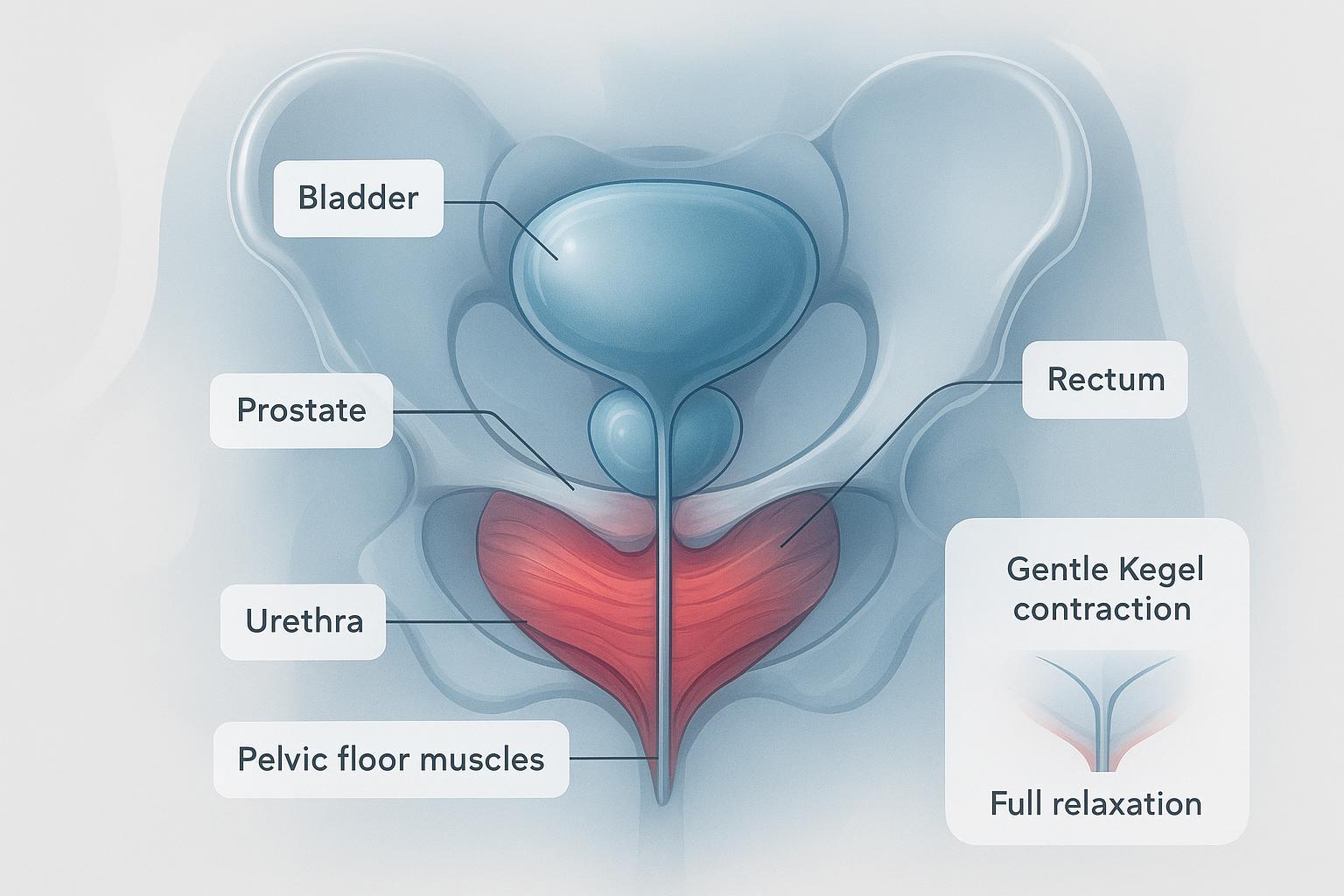
- Pelvic‑floor identification: On an empty bladder, briefly mimic stopping urine midstream to find the right muscles. Then practice 10 gentle squeezes of 3 seconds on and 3 seconds off, breathing normally.
Micro‑example: You reach an 8 out of 10 with a tight grip. You pause, loosen your grip to a 3 out of 10, exhale for 45 seconds, and resume at 5 out of 10. That is a successful cycle.
Weeks 3 to 6 control and consistency
Objective: Add pause–squeeze for near‑climax control, extend edging time, and improve pelvic‑floor coordination.
- Edging sets: Aim for 15 to 20 minutes per session, two or three times weekly. Cycle up to 3 or 4 peaks without ejaculating. If you accidentally climax, log where it happened and keep going next time.
- Pause–squeeze: When you are near climax, gently squeeze just below the ridge of the glans for several seconds until the urge passes, as described by the Mayo Clinic’s patient guidance for behavioral therapy in premature ejaculation: Mayo Clinic behavioral techniques for ejaculation control.
- Pelvic‑floor progression: Build to 3 sets of 10 contractions daily, extending holds to 5 seconds with full 5‑second relaxations. Practice in different positions, and include relaxation breaths between sets.
Micro‑example: Peak two feels stronger than peak one. You add a pause–squeeze for 3 to 4 seconds, then spend a full minute doing slow exhales before resuming.
Weeks 7 to 8 and beyond advanced exploration
Objective: Attempt chaining peaks and, if you wish, explore a non‑ejaculatory orgasm or prostate stimulation with safety in mind.
- Chain peaks: After a strong non‑ejaculatory peak, let arousal dip to 4 to 5, then rise again with lighter strokes or non‑genital touch.
- Optional prostate basics: Start externally with gentle pressure behind the scrotum and around the anus. If you choose internal play, use generous lube, a flared‑base, body‑safe toy, and a condom on the toy if sharing or switching. Stop with pain or bleeding and seek advice if symptoms persist. For barrier and lube compatibility basics, review the CDC’s guidance on condom use and prevention methods: CDC condom use and lubrication guidance.
Micro‑example: After three start–stop cycles, you reach a wave‑like orgasmic sensation without ejaculation. You breathe, let arousal settle, and rebuild slowly toward a second peak.
Technique how‑tos you can practice today
Start–stop method
Objective: Learn to step back from the point of no return and return to a comfortable plateau.
- Build gradually. Increase stimulation until you feel the “about to go over” signal, then stop all stimulation for 30 to 60 seconds while you exhale slowly. Resume at a lower intensity.
- Repeat 2 to 4 times per session. If you ejaculate, that is data. Note the cue you missed and try again in your next session.
Pause–squeeze method
Objective: Interrupt the ejaculatory reflex when you are very close to climax.
- Place a gentle squeeze where the head meets the shaft for several seconds until the urge subsides, as outlined in the Mayo Clinic’s patient guidance on behavioral techniques: patient overview of the pause–squeeze technique.
- Avoid painful force. If you feel soreness, rest 24 to 48 hours.
Pelvic‑floor training for men
- Identify the correct muscles by simulating a brief stop of urine flow or the “hold in gas” cue, then train with relaxed breathing and no buttock, thigh, or abdominal bracing. For a clear how‑to, see the Cleveland Clinic’s patient page on Kegels for men: step‑by‑step Kegels for men.
- Beginner set: 3 seconds on and 3 seconds off × 10 reps, 3 sets per day.
- Progression: Extend to 5 to 10 second holds with equal relax time, and add standing sets. Rest if you feel fatigue or soreness.
Breathwork and tension release
- Keep exhales longer than inhales to downshift arousal. Try 4 seconds in, 6 to 8 seconds out, relaxing the jaw, shoulders, and pelvic floor on each exhale.
- Use breath during every stop phase in start–stop or squeeze cycles.
Sensate focus and non‑genital arousal mapping
- To avoid overstimulating the penis while staying engaged, alternate zones such as chest, thighs, and nipples. For ideas, explore these non‑genital approaches to maintain arousal plateaus in a neutral, educational way on KissSelf — Disclosure: KissSelf is our product — see this primer on non‑genital arousal techniques.
Optional prostate basics with safety
- Begin externally, then consider a small, flared‑base silicone toy with abundant water‑ or silicone‑based lube. Use a condom on the toy if sharing or switching orifices. Clean thoroughly after use. For barrier and lube guidance, see the CDC’s prevention overview and condom pages cited above and the NHS’s overview of sexual activities and risk: NHS sexual health and anal sex risk basics.
Tools that can support practice
Neutral options some readers use to vary sensations or reduce hand fatigue:
- Textured strokers or automatic devices to change intensity and pace. For an educational overview, see KissSelf’s guide to male masturbation techniques and this explainer on automatic strokers and blowjob machines.
- Silicone prostate massagers with a flared base for optional internal practice. Always apply the safety checklist above and review KissSelf’s summary on toy safety and hygiene.
Note: Tools are optional. They do not guarantee results. Keep your framing experimental and patient.
Troubleshooting and quick fixes
- I keep ejaculating during edging: You likely overshot your point of no return. Reduce stimulation earlier, extend the stop phase to 60 seconds with slow exhales, and ease back at half the intensity.
- I feel pelvic‑floor soreness: Scale back reps and hold times for 48 hours. Re‑check that you are fully relaxing between contractions. Consider a pelvic‑floor PT if pain persists.
- Arousal collapses after a stop: Use non‑genital touch and lighter strokes to rebuild to a 4 or 5 before returning to direct stimulation.
- Anal or prostate play is painful: Stop, add more lube, switch to a smaller toy, and go slower. If bleeding or urinary symptoms occur, seek clinical advice.
Technique and evidence summary
| Technique | Purpose | Typical practice | Evidence strength | Key safety notes |
|---|---|---|---|---|
| Start–stop | Learn to descend from pre‑ejaculatory arousal | 2 to 4 cycles per session, 2 to 4 sessions weekly | Behavioral method referenced in the Mayo Clinic’s PE page | Stop if frustrated or in pain, pair with breathwork |
| Pause–squeeze | Interrupt ejaculatory reflex near climax | Gentle squeeze at head–shaft junction for several seconds, repeat as needed | Described by the Mayo Clinic for PE | Avoid painful force, limit repetitions if soreness occurs |
| Kegels for men | Improve pelvic‑floor control | 3 s on and 3 s off × 10 reps, 3 sets daily, progress holds over weeks | Patient education from Cleveland Clinic and Mayo Clinic; supportive reviews | Do not overtrain, relax fully between reps |
| Sensate focus | Maintain arousal without penile overstimulation | Alternate zones to sustain a plateau | General sex‑ed practice; internal resource for ideas | Use lube, stop with discomfort |
| Prostate basics | Optional path to stronger orgasms | External first; if internal, use flared‑base toy, condoms, generous lube | Harm‑reduction guidance from CDC and NHS | Stop with pain or bleeding, clean thoroughly |
Sources mentioned above include the Cleveland Clinic’s sexual response cycle and Kegels pages, the Mayo Clinic’s behavioral guidance for PE, and CDC and NHS harm‑reduction pages.
Session tracker to build the habit
Use this simple table after each session to spot patterns and progress.
| Date | Session type | Drills practiced | Time practiced minutes | Arousal peaks reached | Ejaculation yes or no | Comfort or pain notes | Next adjustment |
|---|---|---|---|---|---|---|---|
| 2026‑02‑__ | Solo | Start–stop 3 cycles, breathwork | 18 | 3 | No | Mild thigh tension, no penile pain | Add pause–squeeze next time |
Tip: Export this layout to a CSV or notes app so you can scan progress over 4 to 8 weeks.
A short video for breath control
When you pause stimulation, controlled breathing helps you come down from the edge. This simple demonstration shows a calm cadence you can adapt: 4‑7‑8 breathing exercise video by Andrew Weil, MD. Keep exhales gentle and longer than inhales.
FAQs on how to have multiple orgasms
- Can men have multiple orgasms without ejaculating
- Some can. Patient education resources define orgasm without semen release in conditions like anejaculation and describe dry orgasms in retrograde ejaculation. Training aims to approach orgasmic peaks without triggering ejaculation. See the Cleveland Clinic’s pages on anejaculation and retrograde ejaculation for definitions.
- How long is the refractory period and can it be shortened
- It varies widely by person and context. Some people can rebuild arousal quickly, while others need significant time. Behavioral practice may help you surf arousal better, but there is no guaranteed way to eliminate the refractory period. See the Cleveland Clinic’s overview of the sexual response cycle and refractory period.
- Is edging safe and how often should I practice
- Edging is generally safe when you avoid pain and do not fixate on performance. Two or three sessions per week with rest days is a reasonable start. If you develop soreness or distress, pause and adjust.
- What role do Kegels play for men trying to have multiple orgasms
- Pelvic‑floor training can improve awareness and control that supports edging and ejaculation delay. Consistency over weeks matters more than intensity. See the Cleveland Clinic’s guide to Kegels for men.
- Is prostate stimulation necessary to have multiple orgasms as a man
- No. Some find prostate play intensifies sensation, but it is optional. If you explore it, follow condom and lubrication guidance and stop with pain. Review the CDC’s condom use basics and the NHS’s sexual health risk overview.
Next steps and gentle reminders
- Keep goals flexible and process‑focused. Improvements often show up within 4 to 8 weeks of regular practice.
- Use the session log to notice trends, and scale stimulation down earlier than you think you need to.
- If you experience persistent pain, urinary changes, erectile or ejaculatory dysfunction, or have post‑surgical questions, consult a clinician.
Looking for how to edge for multiple orgasms in a structured way Start with the foundation weeks above, build consistency, and treat every session as skill practice rather than a test.